Glucose metabolism is a crucial cellular process that produces a significant amount of energy for the cell. When this process is not regulated, it can have adverse effects, including hyperglycemia, high blood pressure, high cholesterol, and increased fat storage. Diabetes mellitus (DM) is the most common disease associated with dysregulated glucose metabolism. Diabetes mellitus is a cluster of chronic metabolic diseases characterized by hyperglycemia and insulin resistance. In 2017, approximately 462 million people worldwide were diagnosed with the disease, and it is currently among the top ten causes of death. While there are several forms of the disease, the two most common forms are Type I and Type II diabetes. Type I diabetes is an autoimmune disease by which immune cells destroy pancreatic beta cells. Pancreatic beta cells secrete insulin, which facilitates glucose uptake in peripheral cells. Insulin deficiency leads to hyperglycemia because the cells are not receiving the signal to uptake glucose. Type I diabetic diagnoses occur during infancy to early childhood years. Type II diabetes is similar to type I diabetes in that both patients experience hyperglycemia. However, type II diabetic patients experience insulin resistance in peripheral tissues. Therefore, even though insulin is present in the body, peripheral cells are desensitized to the signal. Diagnosis of this form of the disease is associated with higher body fat percentage/obesity. Patients around 45 years old receive a diagnosis of the disease. The mechanisms of this disease are enigmatic as the disease’s development comes from both genetic and environmental factors. Furthermore, it is associated with various cardiovascular complications, neuropathies, blindness, obesity, and kidney failure.
Metallomics-centered studies on the disease are looking further into zinc’s novel role in the prognosis of diabetes. Zinc is an essential transition metal that plays a crucial role in several cellular processes, including facilitating catalytic or structural protein function. ZIP (influx) and ZnT (efflux) transporters are responsible for tightly regulating zinc homeostasis. The trace metal plays a vital role in glucose metabolism in that zinc is crucial for the structure and function of insulin. It stabilizes insulin hexamers for storage in pancreatic beta cells, decreases insulin solubility to prevent premature insulin degradation, and enhances insulin binding to hepatocyte membranes.
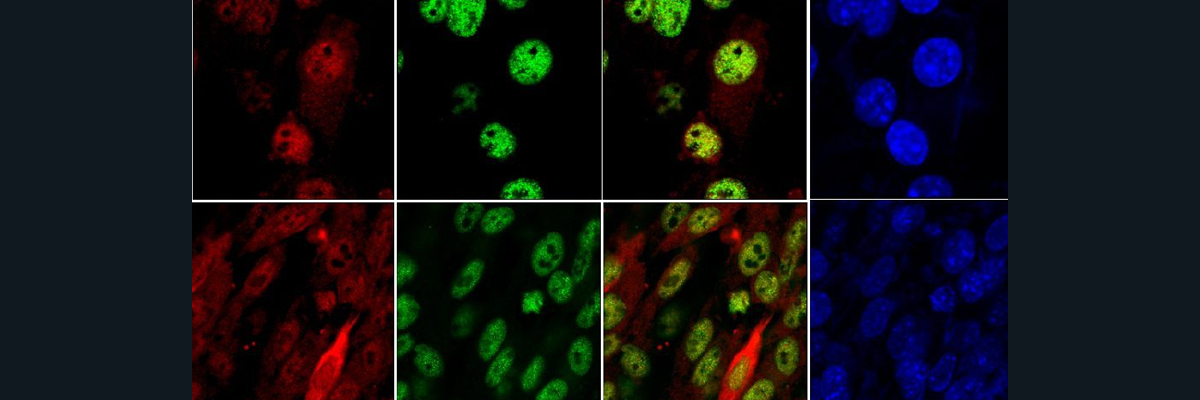
Many diabetic-focused research groups are interested in ZnT8 as this transporter is highly expressed on insulin granules located in pancreatic beta cells. ZnT8 polymorphisms have been linked to type two diabetes. To understand how the compromised function of ZnT8 impacts glucose metabolism and insulin secretion, Wijesekera’s research group conducted ZnT8 knockout (ZnT8KO) experiments in alpha and beta cells in murine models. From these experiments, ZnT8KO in beta cells shows significant glucose intolerance, reduced insulin processing, decreased zinc accumulation in granules, and decreased expression of Pdx1, Mafa, and prohormone processing enzymes. PDX1 and MAFA are transcription factors that bind to the insulin promoter of the DNA and initiate insulin transcription.
As briefly mentioned above, insulin is processed and stored in granules in the pancreatic beta cells. Insulin granules appear dark and dense when crystallized and stored correctly. As a result of improper crystallization and storage, the granules appear lighter, empty, or rod-shaped. ZnT8KO in pancreatic beta cells shows abnormalities in the morphology and number of beta-cell granules. In particular, they were a reduced total number of beta cell granules, including dense-core granules that contain crystallized zinc, thus suggesting that there is a defect in insulin crystallization and packaging. The cells also display an increase in empty, light-core, and rod-shaped granules. There is also a decrease in zinc efflux into immature granules, which leads to incomplete insulin crystallization and granule maturity.
Lastly, insulin secretion occurs in two phases. The first phase occurs approximately two minutes after nutrient ingestion and continues for ten to fifteen minutes. By releasing this hormone, the body is able to absorb fresh nutrients into the bloodstream, suppress gluconeogenesis in the liver, and limit hyperglycemia following the digestion of food. In this study, ZnT8KO in beta-pancreatic cells significantly reduced this first phase response. This reduction is likely due to the fact that there is a decrease in insulin due to the lack of insulin crystallization and granule maturation. Looking through the lens of type II diabetes, I wonder if type two diabetic patients experience gradual insulin deficiency as insulin biosynthesis gets compromised.
The figure below shows a proposed diagram of the insulin biosynthetic pathway in normal and ZnT8KO pancreatic beta-cells. In control cells, insulin biosynthesis begins with PDX1 and MAFA, transcription factors binding to insulin promoter and initiate insulin transcription. The product of this transcript is pre-proinsulin RNA. Pre-proinsulin translocates to endoplasmic reticulum and gets cleaved producing proinsulin. Next, proinsulin transfers to the golgi apparatus, which is a zinc-rich environment, so that it can further get processed and transported into immature insulin granules. Within these granules, cytoplasmic zinc enters the granule through ZnT8. This zinc forms hexamers with proinsulin and C-peptide region gets cleaved by various prohormone processing enzymes to produce mature insulin and complete the crystallization process. With all the findings in this paper, we see how knocking out ZnT8 from pancreatic beta cells produces deleterious effects that contribute to the pathogenesis of diabetes.

Figure 1: Insulin biosynthesis, crystallization and secretion in control and ZnTKO pancreatic beta cells
While these in vivo studies reveal a lot about the importance of ZnT8 in insulin biosynthesis and possible roles in diabetes, more clinical work needs to be done in humans to truly understand ZnT8’s role in the disease. Since ZnT8 polymorphisms have been linked to type II diabetes, it would be interesting to see if the findings presented in this paper would translated if wild type ZnT8 had been swapped with these polymorphisms.
Sources:
Wijesekara, N., Dai, F. F., Hardy, A. B., Giglou, P. R., Bhattacharjee, A., Koshkin, V., Chimienti, F., Gaisano, H. Y., Rutter, G. A., & Wheeler, M. B. (2010). Beta cell-specific ZNT8 deletion in mice causes marked defects in insulin processing, crystallisation and secretion. Diabetologia, 53(8), 1656–1668. https://doi.org/10.1007/s00125-010-1733-9
Arneth, B., Arneth, R., & Shams, M. (2019). Metabolomics of type 1 and type 2 diabetes. International Journal of Molecular Sciences, 20(10), 2467. https://doi.org/10.3390/ijms20102467
Myers, S. A. (2015). Zinc transporters and zinc signaling: New insights into their role in type 2 diabetes. International Journal of Endocrinology, 2015, 1–7. https://doi.org/10.1155/2015/167503